Related Articles
-
Welcome new members from Africa!
PAGH is happy to announce a new partnership with GACOPA and expanding our membership to PAs/Clinical Officers/Clinical Assistants/Health Officers...
-
Adapting Antenatal Care in a Rural LMIC During Covid-19 in Rural Guatemala
Saving Mothers is a 501(c)(3) nonprofit organization dedicated to eradicating preventable maternal deaths and birth-related complications in low-resource settings....
-
New Zealand PA Job Opportunities
International Physician Associate Employment Opportunities Rural Family/General Practice-Emergency Department-Urgent Care New Zealand…… North and South Islands Contract: Full time with...
-
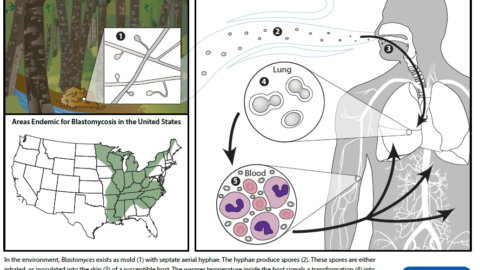
Blastomycosis- Increasing cases reported in Upstate NY
"Blastomycosis is an uncommon and under diagnosed disease typically caused by inhalation of Blastomyces spp. fungi, which grow in...
-
Emergency Deployments to COVID Endemic Regions
Caliburn International Recruiting for immediate deployment to Brooklyn, NY Travel and housing is provided $175/hr + overtime Website for...
-
Webinar: Sunday Sept 8th, PA Profession in Israel
Please join us for our first ever live webinar! Featuring Dr. Oren Berkowitz, PA-C from Ariel University. This event...
-
The Reality of Life: Ob/Gyn Perspectives During COVID-19
These are challenging times, but as healthcare workers we are powering through; working in...
-
Spotlight on International PAs
Series highlighting PAs working around the world. This article is on PA Christopher Casey who works for the U.S....






{kind=link}
0 Comments